What Does Overpronation Mean
Overview
Pes planus is the medical term for flat feet. It comes from Latin, Pes = foot and Planus = plain, level ground. Very few people suffer from this condition, as a true flat foot is very rare. Less than 5% of the population has flat feet. The majority of the population, however, has fallen arches (an estimated 60-70% of the population) known in the medical profession as ?excess pronation? or over-pronation. Over-pronation means the foot and ankle tend to roll inwards and the arch collapses with weight-bearing. This is a quite a destructive position for the foot to function in and may cause a wide variety of foot, leg and lower back conditions.
Causes
In adults, the most common reason for the onset of Over-Pronation is a condition known as Post Tibial Tendonitis. This condition develops from repetitive stress on the main supporting tendon (Posterior Tibial Tendon) of the foot arch. As the body ages, ligaments and muscles can weaken. When this occurs the job of providing the majority of the support required by the foot arch is placed upon this tendon. Unfortunately, this tendon cannot bear the weight of this burden for too long. Eventually it fatigues under the added strain and in doing so the foot arch becomes progressively lower over a period of time.
Symptoms
Overpronation can negatively affect overall body alignment. The lowering of the longitudinal arch pulls the heel bone in, causing the leg, thigh bone and hip to rotate inwards, and an anterior tilt of the pelvis. Unnecessary strain to the ankles, knees, hips and back can result. Plantar fasciitis and inflammation, metatarsal pain, problems with the Achilles tendon, pain on the inside of the knee, and bursitis in the hip are just some of the conditions commonly associated with pronation.
Diagnosis
Pronounced wear on the instep side of shoe heels can indicate overpronation, however it's best to get an accurate assessment. Footbalance retailers offer a free foot analysis to check for overpronation and help you learn more about your feet.
Non Surgical Treatment
Overpronation is a condition in which the foot rolls excessively down and inward. The arch may elongate and collapse (or ?fall?) and the heel will lean inward. Overpronation should not be confused with pronation. Pronation is a normal motion of the foot during weight bearing and allows the foot to absorb shock as it contacts the ground.
Surgical Treatment
Subtalar Arthroereisis. The ankle and hindfoot bones/midfoot bones around the joint are fused, locking the bones in place and preventing all joint motion. This may also be done in combination with fusion at other joints. This is a very aggressive option usually reserved for extreme cases where no joint flexibility is present and/or the patient has severe arthritic changes in the joint.
Pes planus is the medical term for flat feet. It comes from Latin, Pes = foot and Planus = plain, level ground. Very few people suffer from this condition, as a true flat foot is very rare. Less than 5% of the population has flat feet. The majority of the population, however, has fallen arches (an estimated 60-70% of the population) known in the medical profession as ?excess pronation? or over-pronation. Over-pronation means the foot and ankle tend to roll inwards and the arch collapses with weight-bearing. This is a quite a destructive position for the foot to function in and may cause a wide variety of foot, leg and lower back conditions.
Causes
In adults, the most common reason for the onset of Over-Pronation is a condition known as Post Tibial Tendonitis. This condition develops from repetitive stress on the main supporting tendon (Posterior Tibial Tendon) of the foot arch. As the body ages, ligaments and muscles can weaken. When this occurs the job of providing the majority of the support required by the foot arch is placed upon this tendon. Unfortunately, this tendon cannot bear the weight of this burden for too long. Eventually it fatigues under the added strain and in doing so the foot arch becomes progressively lower over a period of time.
Symptoms
Overpronation can negatively affect overall body alignment. The lowering of the longitudinal arch pulls the heel bone in, causing the leg, thigh bone and hip to rotate inwards, and an anterior tilt of the pelvis. Unnecessary strain to the ankles, knees, hips and back can result. Plantar fasciitis and inflammation, metatarsal pain, problems with the Achilles tendon, pain on the inside of the knee, and bursitis in the hip are just some of the conditions commonly associated with pronation.
Diagnosis
Pronounced wear on the instep side of shoe heels can indicate overpronation, however it's best to get an accurate assessment. Footbalance retailers offer a free foot analysis to check for overpronation and help you learn more about your feet.
Non Surgical Treatment
Overpronation is a condition in which the foot rolls excessively down and inward. The arch may elongate and collapse (or ?fall?) and the heel will lean inward. Overpronation should not be confused with pronation. Pronation is a normal motion of the foot during weight bearing and allows the foot to absorb shock as it contacts the ground.
Surgical Treatment
Subtalar Arthroereisis. The ankle and hindfoot bones/midfoot bones around the joint are fused, locking the bones in place and preventing all joint motion. This may also be done in combination with fusion at other joints. This is a very aggressive option usually reserved for extreme cases where no joint flexibility is present and/or the patient has severe arthritic changes in the joint.
Physiotherapy For Calcaneal Apophysitis
Overview
Severs disease, also known as calcaneal apophysitis, is a condition in which the growth plate along the heel becomes inflamed. It most commonly occurs in active, early-teen children. Most patients with Severs disease complain of heel pain. In general the pain is exacerbated with increased activities, such as running, jumping, or climbing stairs. The pain often improves with a period of rest.
Causes
During the growth spurt of early puberty, the heel bone (also called the calcaneus) sometimes grows faster than the leg muscles and tendons. This can cause the muscles and tendons to become very tight and overstretched, making the heel less flexible and putting pressure on the growth plate. The Achilles tendon (also called the heel cord) is the strongest tendon that attaches to the growth plate in the heel. Over time, repeated stress (force or pressure) on the already tight Achilles tendon damages the growth plate, causing the swelling, tenderness, and pain of Sever's disease. Such stress commonly results from physical activities and sports that involve running and jumping, especially those that take place on hard surfaces, such as track, basketball, soccer, and gymnastics.
Symptoms
The typical clinical presentation is an active child (aged 9-10 years) who complains of pain at the posterior heel that is made worse by sports, especially those involving running or jumping. The onset is usually gradual. Often, the pain has been relieved somewhat with rest and consequently has been patiently monitored by the patient, parents, coaches, trainers, and family physicians, in the expectation that it will resolve. When the pain continues to interfere with sports performance and then with daily activities, further consultation is sought. It should be kept in mind that failure to instruct patients and parents that continual pain, significant swelling or redness, and fever are not signs of Sever disease and therefore require further evaluation could result in failure to diagnose a condition with much more serious long-term consequences.
Diagnosis
Radiography. Most of the time radiographs are not helpful because the calcaneal apophysis is frequently fragmented and dense in normal children. But they can be used to exclude other traumas. Ultrasonography. could show the fragmentation of secondary nucleus of ossification of the calcaneus in severs?s disease. This is a safe diagnostic tool since there is no radiation. This diagnostic tool can also be used to exclude Achilles tendinitis and/or retrocalcaneal bursitis.
Non Surgical Treatment
The treatment of Sever's disease should be individualized. The most important first steps in the treatment of Sever's disease are activity modification (including rest and sometimes crutches) and good shoes. Further treatment may include icing to decrease pain around the calcaneal apophysis, stretching and strengthening exercises, shoe orthotics or medications to relieve pain. Rarely, a removable cast is necessary to completely rest the foot.
Severs disease, also known as calcaneal apophysitis, is a condition in which the growth plate along the heel becomes inflamed. It most commonly occurs in active, early-teen children. Most patients with Severs disease complain of heel pain. In general the pain is exacerbated with increased activities, such as running, jumping, or climbing stairs. The pain often improves with a period of rest.
Causes
During the growth spurt of early puberty, the heel bone (also called the calcaneus) sometimes grows faster than the leg muscles and tendons. This can cause the muscles and tendons to become very tight and overstretched, making the heel less flexible and putting pressure on the growth plate. The Achilles tendon (also called the heel cord) is the strongest tendon that attaches to the growth plate in the heel. Over time, repeated stress (force or pressure) on the already tight Achilles tendon damages the growth plate, causing the swelling, tenderness, and pain of Sever's disease. Such stress commonly results from physical activities and sports that involve running and jumping, especially those that take place on hard surfaces, such as track, basketball, soccer, and gymnastics.
Symptoms
The typical clinical presentation is an active child (aged 9-10 years) who complains of pain at the posterior heel that is made worse by sports, especially those involving running or jumping. The onset is usually gradual. Often, the pain has been relieved somewhat with rest and consequently has been patiently monitored by the patient, parents, coaches, trainers, and family physicians, in the expectation that it will resolve. When the pain continues to interfere with sports performance and then with daily activities, further consultation is sought. It should be kept in mind that failure to instruct patients and parents that continual pain, significant swelling or redness, and fever are not signs of Sever disease and therefore require further evaluation could result in failure to diagnose a condition with much more serious long-term consequences.
Diagnosis
Radiography. Most of the time radiographs are not helpful because the calcaneal apophysis is frequently fragmented and dense in normal children. But they can be used to exclude other traumas. Ultrasonography. could show the fragmentation of secondary nucleus of ossification of the calcaneus in severs?s disease. This is a safe diagnostic tool since there is no radiation. This diagnostic tool can also be used to exclude Achilles tendinitis and/or retrocalcaneal bursitis.
Non Surgical Treatment
The treatment of Sever's disease should be individualized. The most important first steps in the treatment of Sever's disease are activity modification (including rest and sometimes crutches) and good shoes. Further treatment may include icing to decrease pain around the calcaneal apophysis, stretching and strengthening exercises, shoe orthotics or medications to relieve pain. Rarely, a removable cast is necessary to completely rest the foot.
Causes Of Acquired Flat Foot
Overview
The adult acquired flatfoot (AAF) is a progressive, symptomatic (painful) deformity resulting from gradual stretch (attenuation) of the tibialis posterior tendon as well as the ligaments that support the arch of the foot. Although the posterior tibialis tendon plays a significant role, this pathology has recently been recognized as involving failure of other interosseous ligaments, such as the spring ligament. Due to the complexity of this pathology, posterior tibial tendon dysfunction (PTTD) is now referred to as adult acquired flatfoot. Severe flatfoot associated with AAF can lead to other problems, such as plantar fascial tension, tendon pain, rearfoot subluxation, and ankle osteoarthritis. 
Causes
As the name suggests, adult-acquired flatfoot occurs once musculoskeletal maturity is reached, and it can present for a number of reasons, though one stands out among the others. While fractures, dislocations, tendon lacerations, and other such traumatic events do contribute to adult-acquired flatfoot as a significant lower extremity disorder, as mentioned above, damage to the posterior tibial tendon is most often at the heart of adult-acquired flatfoot. One study further elaborates on the matter by concluding that ?60% of patients [presenting with posterior tibial tendon damage and adult-acquired flatfoot] were obese or had diabetes mellitus, hypertension, previous surgery or trauma to the medial foot, or treatment with steroids?.
Symptoms
The types of symptoms that may indicate Adult-Acquired Flat Foot Deformity include foot pain that worsens over time, loss of the arch, abnormal shoe wear (excessive wearing on the inner side of shoe from walking on the inner side of the foot) and an awkward appearance of the foot and ankle (when viewed from behind, heel and toes appear to go out to the side). It is important that we help individuals recognize the early symptoms of this condition, as there are many treatment options, depending upon the severity, the age of the patient, and the desired activity levels.
Diagnosis
Starting from the knee down, check for any bowing of the tibia. A tibial varum will cause increased medial stress on the foot and ankle. This is essential to consider in surgical planning. Check the gastrocnemius muscle and Achilles complex via a straight and bent knee check for equinus. If the range of motion improves to at least neutral with bent knee testing of the Achilles complex, one may consider a gastrocnemius recession. If the Achilles complex is still tight with bent knee testing, an Achilles lengthening may be necessary. Check the posterior tibial muscle along its entire course. Palpate the muscle and observe the tendon for strength with a plantarflexion and inversion stress test. Check the flexor muscles for strength in order to see if an adequate transfer tendon is available. Check the anterior tibial tendon for size and strength.
Non surgical Treatment
Conservative treatment is indicated for nearly all patients initially before surgical management is considered. The key factors in determining appropriate treatment are whether acute inflammation and whether the foot deformity is flexible or fixed. However, the ultimate treatment is often determined by the patients, most of whom are women aged 40 or older. Compliance can be a problem, especially in stages I and II. It helps to emphasise to the patients that tibialis posterior dysfunction is a progressive and chronic condition and that several fittings and a trial of several different orthoses or treatments are often needed before a tolerable treatment is found. 
Surgical Treatment
Types of surgery your orthopaedist may discuss with you include arthrodesis, or welding (fusing) one or more of the bones in the foot/ankle together. Osteotomy, or cutting and reshaping a bone to correct alignment. Excision, or removing a bone or bone spur. Synovectomy, or cleaning the sheath covering a tendon. Tendon transfer, or using a piece of one tendon to lengthen or replace another. Having flat feet is a serious matter. If you are experiencing foot pain and think it may be related to flat feet, talk to your orthopaedist.
Adult Aquired FlatFoot
Overview
One in four adults in the U.S. has adult acquired flatfoot deformity, which may begin during childhood or be acquired with age. The foot may be flat all the time or may lose its arch when the person stands. The most common and serious cause of flat foot is Posterior Tibial Tendon Dysfunction, in which the main tendon that supports the arch gradually weakens.
Causes
As discussed above, many health conditions can create a painful flatfoot. Damage to the posterior tibial tendon is the most common cause of AAFD. The posterior tibial tendon is one of the most important tendons of the leg. It starts at a muscle in the calf, travels down the inside of the lower leg and attaches to the bones on the inside of the foot. The main function of this tendon is to hold up the arch and support your foot when you walk. If the tendon becomes inflamed or torn, the arch will slowly collapse. Women and people over 40 are more likely to develop problems with the posterior tibial tendon. Other risk factors include obesity, diabetes, and hypertension. Having flat feet since childhood increases the risk of developing a tear in the posterior tibial tendon. In addition, people who are involved in high impact sports, such as basketball, tennis, or soccer, may have tears of the tendon from repetitive use. Inflammatory arthritis, such as rheumatoid arthritis, can cause a painful flatfoot. This type of arthritis attacks not only the cartilage in the joints, but also the ligaments that support the foot. Inflammatory arthritis not only causes pain, but also causes the foot to change shape and become flat. The arthritis can affect the back of the foot or the middle of foot, both of which can result in a fallen arch.
Symptoms
Depending on the cause of the flatfoot, a patient may experience one or more of the different symptoms here. Pain along the course of the posterior tibial tendon which lies on the inside of the foot and ankle. This can be associated with swelling on the inside of the ankle. Pain that is worse with activity. High intensity or impact activities, such as running, can be very difficult. Some patients can have difficulty walking or even standing for long periods of time. When the foot collapses, the heel bone may shift position and put pressure on the outside ankle bone (fibula). This can cause pain on the outside of the ankle. Arthritis in the heel also causes this same type of pain. Patients with an old injury or arthritis in the middle of the foot can have painful, bony bumps on the top and inside of the foot. These make shoewear very difficult. Occasionally, the bony spurs are so large that they pinch the nerves which can result in numbness and tingling on the top of the foot and into the toes. Diabetics may only notice swelling or a large bump on the bottom of the foot. Because their sensation is affected, people with diabetes may not have any pain. The large bump can cause skin problems and an ulcer (a sore that does not heal) may develop if proper diabetic shoewear is not used.
Diagnosis
In the early stages of dysfunction of the posterior tibial tendon, most of the discomfort is located medially along the course of the tendon and the patient reports fatigue and aching on the plantar-medial aspect of the foot and ankle. Swelling is common if the dysfunction is associated with tenosynovitis. As dysfunction of the tendon progresses, maximum pain occurs laterally in the sinus tarsi because of impingement of the fibula against the calcaneus. With increasing deformity, patients report that the shape of the foot changes and that it becomes increasingly difficult to wear shoes. Many patients no longer report pain in the medial part of the foot and ankle after a complete rupture of the posterior tibial tendon has occurred; instead, the pain is located laterally. If a fixed deformity has not occurred, the patient may report that standing or walking with the hindfoot slightly inverted alleviates the lateral impingement and relieves the pain in the lateral part of the foot.
Non surgical Treatment
Conservative treatment is indicated for nearly all patients initially before surgical management is considered. The key factors in determining appropriate treatment are whether acute inflammation and whether the foot deformity is flexible or fixed. However, the ultimate treatment is often determined by the patients, most of whom are women aged 40 or older. Compliance can be a problem, especially in stages I and II. It helps to emphasise to the patients that tibialis posterior dysfunction is a progressive and chronic condition and that several fittings and a trial of several different orthoses or treatments are often needed before a tolerable treatment is found.

Surgical Treatment
Surgery is usually performed when non-surgical measures have failed. The goal of surgery is to eliminate pain, stop progression of the deformity and improve a patient?s mobility. More than one technique may be used, and surgery tends to include one or more of the following. The tendon is reconstructed or replaced using another tendon in the foot or ankle The name of the technique depends on the tendon used. Flexor digitorum longus (FDL) transfer. Flexor hallucis longus (FHL) transfer. Tibialis anterior transfer (Cobb procedure). Calcaneal osteotomy - the heel bone may be shifted to bring your heel back under your leg and the position fixed with a screw. Lengthening of the Achilles tendon if it is particularly tight. Repair one of the ligaments under your foot. If you smoke, your surgeon may refuse to operate unless you can refrain from smoking before and during the healing phase of your procedure. Research has proven that smoking delays bone healing significantly.
One in four adults in the U.S. has adult acquired flatfoot deformity, which may begin during childhood or be acquired with age. The foot may be flat all the time or may lose its arch when the person stands. The most common and serious cause of flat foot is Posterior Tibial Tendon Dysfunction, in which the main tendon that supports the arch gradually weakens.
Causes
As discussed above, many health conditions can create a painful flatfoot. Damage to the posterior tibial tendon is the most common cause of AAFD. The posterior tibial tendon is one of the most important tendons of the leg. It starts at a muscle in the calf, travels down the inside of the lower leg and attaches to the bones on the inside of the foot. The main function of this tendon is to hold up the arch and support your foot when you walk. If the tendon becomes inflamed or torn, the arch will slowly collapse. Women and people over 40 are more likely to develop problems with the posterior tibial tendon. Other risk factors include obesity, diabetes, and hypertension. Having flat feet since childhood increases the risk of developing a tear in the posterior tibial tendon. In addition, people who are involved in high impact sports, such as basketball, tennis, or soccer, may have tears of the tendon from repetitive use. Inflammatory arthritis, such as rheumatoid arthritis, can cause a painful flatfoot. This type of arthritis attacks not only the cartilage in the joints, but also the ligaments that support the foot. Inflammatory arthritis not only causes pain, but also causes the foot to change shape and become flat. The arthritis can affect the back of the foot or the middle of foot, both of which can result in a fallen arch.
Symptoms
Depending on the cause of the flatfoot, a patient may experience one or more of the different symptoms here. Pain along the course of the posterior tibial tendon which lies on the inside of the foot and ankle. This can be associated with swelling on the inside of the ankle. Pain that is worse with activity. High intensity or impact activities, such as running, can be very difficult. Some patients can have difficulty walking or even standing for long periods of time. When the foot collapses, the heel bone may shift position and put pressure on the outside ankle bone (fibula). This can cause pain on the outside of the ankle. Arthritis in the heel also causes this same type of pain. Patients with an old injury or arthritis in the middle of the foot can have painful, bony bumps on the top and inside of the foot. These make shoewear very difficult. Occasionally, the bony spurs are so large that they pinch the nerves which can result in numbness and tingling on the top of the foot and into the toes. Diabetics may only notice swelling or a large bump on the bottom of the foot. Because their sensation is affected, people with diabetes may not have any pain. The large bump can cause skin problems and an ulcer (a sore that does not heal) may develop if proper diabetic shoewear is not used.
Diagnosis
In the early stages of dysfunction of the posterior tibial tendon, most of the discomfort is located medially along the course of the tendon and the patient reports fatigue and aching on the plantar-medial aspect of the foot and ankle. Swelling is common if the dysfunction is associated with tenosynovitis. As dysfunction of the tendon progresses, maximum pain occurs laterally in the sinus tarsi because of impingement of the fibula against the calcaneus. With increasing deformity, patients report that the shape of the foot changes and that it becomes increasingly difficult to wear shoes. Many patients no longer report pain in the medial part of the foot and ankle after a complete rupture of the posterior tibial tendon has occurred; instead, the pain is located laterally. If a fixed deformity has not occurred, the patient may report that standing or walking with the hindfoot slightly inverted alleviates the lateral impingement and relieves the pain in the lateral part of the foot.
Non surgical Treatment
Conservative treatment is indicated for nearly all patients initially before surgical management is considered. The key factors in determining appropriate treatment are whether acute inflammation and whether the foot deformity is flexible or fixed. However, the ultimate treatment is often determined by the patients, most of whom are women aged 40 or older. Compliance can be a problem, especially in stages I and II. It helps to emphasise to the patients that tibialis posterior dysfunction is a progressive and chronic condition and that several fittings and a trial of several different orthoses or treatments are often needed before a tolerable treatment is found.
Surgical Treatment
Surgery is usually performed when non-surgical measures have failed. The goal of surgery is to eliminate pain, stop progression of the deformity and improve a patient?s mobility. More than one technique may be used, and surgery tends to include one or more of the following. The tendon is reconstructed or replaced using another tendon in the foot or ankle The name of the technique depends on the tendon used. Flexor digitorum longus (FDL) transfer. Flexor hallucis longus (FHL) transfer. Tibialis anterior transfer (Cobb procedure). Calcaneal osteotomy - the heel bone may be shifted to bring your heel back under your leg and the position fixed with a screw. Lengthening of the Achilles tendon if it is particularly tight. Repair one of the ligaments under your foot. If you smoke, your surgeon may refuse to operate unless you can refrain from smoking before and during the healing phase of your procedure. Research has proven that smoking delays bone healing significantly.
Achilles Tendonitis Causes And Treatments
Overview
 Achilles tendinitis is when the tendon that connects the back of your leg to your heel becomes swollen and painful near the bottom of the foot. This tendon is called the Achilles tendon. It is used for walking, running, and jumping.
Achilles tendinitis is when the tendon that connects the back of your leg to your heel becomes swollen and painful near the bottom of the foot. This tendon is called the Achilles tendon. It is used for walking, running, and jumping.
Causes
Tendinitis can result from an injury or over-use. Improper stretching prior to exertion or incorrect form during physical activity can also contribute to the development of tendinitis. Some people, including those with ?flat feet,? tight tendons or arthritis, are particularly prone to tendinitis.
Symptoms
Pain anywhere along the tendon, but most often on or close to the heel. Swelling of the skin over the tendon, associated with warmth, redness and tenderness. Pain on rising up on the toes and pain with pushing off on the toes. If you are unable to stand on your toes you may have ruptured the tendon. This requires urgent medical attention. A painful heel for the first few minutes of walking after waking up in the morning. Stiffness of the ankle, which often improves with mild activity.
Diagnosis
During an examination of the foot and ankle, you doctor will look for the following signs, Achilles tendon swelling or thickening. Bone spurs appearing at the lower part of the tendon at the back of the hell. Pain at the middle or lower area of the Achilles tendon. Limited range of motion of the foot and ankle, and a decreased ability to flex the foot. Your doctor may perform imaging tests, such as X-rays and MRI scans, to make a diagnosis of Achilles tendinitis. X-rays show images of the bones and can help the physician to determine if the Achilles tendon has become hardened, which indicated insertional Achilles tendinitis. MRI scans may not be necessary, but they are important guides if you are recommended to have surgical treatment. An MRI can show the severity of the damage and determine what kind of procedure would be best to address the condition.
Nonsurgical Treatment
The main treatments for Achilles tendinitis do not involve surgery. It is important to remember that it may take at least 2 to 3 months for the pain to go away. Try putting ice over the Achilles tendon for 15 to 20 minutes, two to three times per day. Remove the ice if the area gets numb. Changes in activity may help manage the symptoms. Decrease or stop any activity that causes you pain. Run or walk on smoother and softer surfaces. Switch to biking, swimming, or other activities that put less stress on the Achilles tendon. Your health care provider or physical therapist can show you stretching exercises for the Achilles tendon. They may also suggest the following changes in your footwear, a brace or boot or cast to keep the heel and tendon still and allow the swelling to go down, heel lifts placed in the shoe under the heel, shoes that are softer in the areas over and under the heel cushion. Nonsteroidal anti-inflammatory drugs (NSAIDs) such as aspirin and ibuprofen can help with pain or swelling. Talk with your health care provider. If these treatments do not improve symptoms, you may need surgery to remove inflamed tissue and abnormal areas of the tendon. Surgery also can be used to remove the bone spur that is irritating the tendon. Extracorporeal shock wave therapy (ESWT) may be an alternative to surgery for people who have not responded to other treatments. This treatment uses low-dose sound waves.
Surgical Treatment
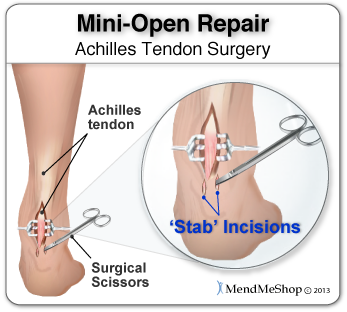
Surgery is considered the last resort. It is only recommended if all other treatment options have failed after at least six months. In this situation, badly damaged portions of the tendon may be removed. If the tendon has ruptured, surgery is necessary to re-attach the tendon. Rehabilitation, including stretching and strength exercises, is started soon after the surgery. In most cases, normal activities can be resumed after about 10 weeks. Return to competitive sport for some people may be delayed for about three to six months.
Prevention
The following measures can significantly reduce the risk of developing Achilles tendonitis. Adequately stretch and warm up prior to exercise. Warm down and stretch after exercise. Choose footwear carefully and use footwear appropriate to the sport being undertaken. Use orthotic devices in footwear to correctly support the foot. Exercise within fitness levels and follow a sensible exercise programme. Develop strong, flexible calf muscles.
Achilles tendinitis is when the tendon that connects the back of your leg to your heel becomes swollen and painful near the bottom of the foot. This tendon is called the Achilles tendon. It is used for walking, running, and jumping.
Causes
Tendinitis can result from an injury or over-use. Improper stretching prior to exertion or incorrect form during physical activity can also contribute to the development of tendinitis. Some people, including those with ?flat feet,? tight tendons or arthritis, are particularly prone to tendinitis.
Symptoms
Pain anywhere along the tendon, but most often on or close to the heel. Swelling of the skin over the tendon, associated with warmth, redness and tenderness. Pain on rising up on the toes and pain with pushing off on the toes. If you are unable to stand on your toes you may have ruptured the tendon. This requires urgent medical attention. A painful heel for the first few minutes of walking after waking up in the morning. Stiffness of the ankle, which often improves with mild activity.
Diagnosis
During an examination of the foot and ankle, you doctor will look for the following signs, Achilles tendon swelling or thickening. Bone spurs appearing at the lower part of the tendon at the back of the hell. Pain at the middle or lower area of the Achilles tendon. Limited range of motion of the foot and ankle, and a decreased ability to flex the foot. Your doctor may perform imaging tests, such as X-rays and MRI scans, to make a diagnosis of Achilles tendinitis. X-rays show images of the bones and can help the physician to determine if the Achilles tendon has become hardened, which indicated insertional Achilles tendinitis. MRI scans may not be necessary, but they are important guides if you are recommended to have surgical treatment. An MRI can show the severity of the damage and determine what kind of procedure would be best to address the condition.
Nonsurgical Treatment
The main treatments for Achilles tendinitis do not involve surgery. It is important to remember that it may take at least 2 to 3 months for the pain to go away. Try putting ice over the Achilles tendon for 15 to 20 minutes, two to three times per day. Remove the ice if the area gets numb. Changes in activity may help manage the symptoms. Decrease or stop any activity that causes you pain. Run or walk on smoother and softer surfaces. Switch to biking, swimming, or other activities that put less stress on the Achilles tendon. Your health care provider or physical therapist can show you stretching exercises for the Achilles tendon. They may also suggest the following changes in your footwear, a brace or boot or cast to keep the heel and tendon still and allow the swelling to go down, heel lifts placed in the shoe under the heel, shoes that are softer in the areas over and under the heel cushion. Nonsteroidal anti-inflammatory drugs (NSAIDs) such as aspirin and ibuprofen can help with pain or swelling. Talk with your health care provider. If these treatments do not improve symptoms, you may need surgery to remove inflamed tissue and abnormal areas of the tendon. Surgery also can be used to remove the bone spur that is irritating the tendon. Extracorporeal shock wave therapy (ESWT) may be an alternative to surgery for people who have not responded to other treatments. This treatment uses low-dose sound waves.
Surgical Treatment
Surgery is considered the last resort. It is only recommended if all other treatment options have failed after at least six months. In this situation, badly damaged portions of the tendon may be removed. If the tendon has ruptured, surgery is necessary to re-attach the tendon. Rehabilitation, including stretching and strength exercises, is started soon after the surgery. In most cases, normal activities can be resumed after about 10 weeks. Return to competitive sport for some people may be delayed for about three to six months.
Prevention
The following measures can significantly reduce the risk of developing Achilles tendonitis. Adequately stretch and warm up prior to exercise. Warm down and stretch after exercise. Choose footwear carefully and use footwear appropriate to the sport being undertaken. Use orthotic devices in footwear to correctly support the foot. Exercise within fitness levels and follow a sensible exercise programme. Develop strong, flexible calf muscles.
Indicators And Treatment For Diabetic Foot
There is no one treatment that works well for all diabetics. Silver sulfadiazine cream causes a temporary skin discoloration around the ulcer site, which is considered normal. But at its annual Diabetes Professional Conference, which kicked off today in Liverpool, the charity group warned that many of the 6,000 diabetes-related amputations that occur each year are the result of a lack of awareness of the symptoms and treatment of diabetic foot problems , as well as poor services. Many people are being left in the dark about what to look for and when to seek medical help, meaning those who develop foot disease often suffer in silence for months. As a result, treatment is often delayed for months, thus lowering the patient's chances of saving their foot. In addition, 15% of diabetics do not have an annual foot examination , while others get a check but are not told whether they are at high risk of foot disease. Foot tattoos look really attractive since they are placed on a flat surface.

The delayed- or non-healing of wounds is one of the major diabetes complications that cause suffering in people with diabetes and results in more than 500,000 new diabetic foot ulcers and 50,000 lower extremity amputations per year in the US alone. University of Notre Dame researchers have, for the first time, identified the enzymes that are detrimental to diabetic wound healing and those that are beneficial to repair the wound. On the other hand, type 2 diabetes is said to occur in middle-aged and the elderly, who suffer from problems in relation to obesity. Though most women experience these symptoms, in many cases, people suffering from type II diabetes do not experience any symptom for years. Usually, type 2 diabetes is diagnosed after serious health problems, like heart attacks, or vision problems arise. The International Symposium on the Diabetic Foot has become the standard international (scientific) meeting on this topic.
There is in this case, a problem for the diabetic in telling the difference between sharp pain and a more dull pain. Consequently major cuts and wounds often go undetected and diabetic foot ulcers can become problematic. However without effective feedback from the nerves in your foot ot toe, then that adjustment is not adequately made.
Diabetic foot ulcers as one of the most common complications of diabetes mellitus are defined as nonhealing or long-lasting chronic skin ulcers in diabetic patients. Low level laser therapy (LLLT) on wound areas as well as on acupuncture points, as a noninvasive, pain-free method with minor side effects, has been considered as a possible treatment option for the diabetic foot syndrome. The majority of clinical studies show a potential benefit of LLLT in wound healing of diabetic ulcers.
The prevalence of peripheral vascular disease was 15%, hallux vulgus was 22.5%, inappropriate foot wear was 41%, and peripheral neuropathy was 47.5%. Peripheral neuropathy and inappropriate foot wear were the most common risk factors for foot ulceration. Foot ulceration, secondary to diabetes, is the most common reason for lower limb amputation, accounting for 50-70% of non-traumatic lower limb amputations. Rather than progressing through the usual wound healing phases, diabetic wounds become ‘stuck', predominantly in the inflammatory phase. Chronic diabetic wounds always have a bacterial load, and the increased tissue bacterial burden may impede healing. This review seeks to examine factors that prevent diabetic wound healing and the potential of four bee products to promote diabetic human healing in these wounds. Anyone who has diabetes can develop a foot ulcer.
A physical therapist will teach a patient exercises and use specific modalities to help improve symptoms, increase muscle strength and improve control. Therefore, a patient should be Hallux Valgus sure to attend all physical therapy sessions in order to gain the maximum benefit for peripheral neuropathy. Peripheral neuropathy denotes damage to nerve endings in our extremities.
The delayed- or non-healing of wounds is one of the major diabetes complications that cause suffering in people with diabetes and results in more than 500,000 new diabetic foot ulcers and 50,000 lower extremity amputations per year in the US alone. University of Notre Dame researchers have, for the first time, identified the enzymes that are detrimental to diabetic wound healing and those that are beneficial to repair the wound. On the other hand, type 2 diabetes is said to occur in middle-aged and the elderly, who suffer from problems in relation to obesity. Though most women experience these symptoms, in many cases, people suffering from type II diabetes do not experience any symptom for years. Usually, type 2 diabetes is diagnosed after serious health problems, like heart attacks, or vision problems arise. The International Symposium on the Diabetic Foot has become the standard international (scientific) meeting on this topic.
There is in this case, a problem for the diabetic in telling the difference between sharp pain and a more dull pain. Consequently major cuts and wounds often go undetected and diabetic foot ulcers can become problematic. However without effective feedback from the nerves in your foot ot toe, then that adjustment is not adequately made.
Diabetic foot ulcers as one of the most common complications of diabetes mellitus are defined as nonhealing or long-lasting chronic skin ulcers in diabetic patients. Low level laser therapy (LLLT) on wound areas as well as on acupuncture points, as a noninvasive, pain-free method with minor side effects, has been considered as a possible treatment option for the diabetic foot syndrome. The majority of clinical studies show a potential benefit of LLLT in wound healing of diabetic ulcers.
The prevalence of peripheral vascular disease was 15%, hallux vulgus was 22.5%, inappropriate foot wear was 41%, and peripheral neuropathy was 47.5%. Peripheral neuropathy and inappropriate foot wear were the most common risk factors for foot ulceration. Foot ulceration, secondary to diabetes, is the most common reason for lower limb amputation, accounting for 50-70% of non-traumatic lower limb amputations. Rather than progressing through the usual wound healing phases, diabetic wounds become ‘stuck', predominantly in the inflammatory phase. Chronic diabetic wounds always have a bacterial load, and the increased tissue bacterial burden may impede healing. This review seeks to examine factors that prevent diabetic wound healing and the potential of four bee products to promote diabetic human healing in these wounds. Anyone who has diabetes can develop a foot ulcer.
A physical therapist will teach a patient exercises and use specific modalities to help improve symptoms, increase muscle strength and improve control. Therefore, a patient should be Hallux Valgus sure to attend all physical therapy sessions in order to gain the maximum benefit for peripheral neuropathy. Peripheral neuropathy denotes damage to nerve endings in our extremities.
What Exactly Triggers Heel Discomfort
Overview
Plantar fasciitis is a condition characterised by damage and inflammation to the plantar fascia (i.e. the connective tissue on the sole of the foot forming the inner arch. This usually occurs at the attachment of the plantar fascia to the heel bone. Plantar fasciitis is the most common cause of heel pain seen in clinical practice. During walking or running, tension is placed through the plantar fascia. When this tension is excessive (often due to poor foot biomechanics such as flat feet or if it is too repetitive or forceful, damage to the plantar fascia can occur. Plantar fasciitis is a condition where there is damage to the plantar fascia with subsequent inflammation and degeneration. This may occur traumatically due to a high force going through the plantar fascia beyond what it can withstand or, more commonly, due to gradual wear and tear associated with overuse. Occasionally, a heel spur may develop in association with plantar fasciitis.
Causes
You are at a greater risk for developing plantar fasciitis if you are overweight or obese. This is due to the increased pressure on your plantar fascia ligaments, especially if you have sudden weight gain. Women who are pregnant often experience bouts of plantar fasciitis, particularly during late pregnancy. If you are a long distance runner, you may be more likely to develop plantar fascia problems. You are also at risk if you have a very active job that involves being on your feet often, such as a factory worker or a restaurant server. Active men and women between the ages of 40 and 70 are at the highest risk for developing plantar fasciitis. It is also slightly more common in women than men. If you have foot problems, such as very high arches or very flat feet, you may develop plantar fasciitis. Tight Achilles tendons (the tendons attaching the calf muscles to the heels) may also result in plantar fascia pain. Simply wearing shoes with soft soles and poor arch support can also result in plantar fasciitis. Plantar fasciitis is not caused by heel spurs. A heel spur is a hook of bone that can form on the heel bone (calcaneus) of the foot. One out of every 10 people has a heel spur, but only one out of 20 people with heel spurs experience pain, according to OrthoInfo.
Symptoms
People with this condition sometimes describe the feeling as a hot, sharp sensation in the heel. You usually notice the pain first thing in the morning when you stand. After walking for a period of time, the pain usually lessens or even disappears. However, sharp pain in the center of the heel may return after resting for a period of time and then resuming activity.
Diagnosis
Your doctor will check your feet and watch you stand and walk. He or she will also ask questions about your past health, including what illnesses or injuries you have had. Your symptoms, such as where the pain is and what time of day your foot hurts most. How active you are and what types of physical activity you do. Your doctor may take an X-ray of your foot if he or she suspects a problem with the bones of your foot, such as a stress fracture.
Non Surgical Treatment
To alleviate the stress and pain on the fascia, the person can take shorter steps and avoid walking barefoot. Activities that involve foot impact, such as jogging, should be avoided. The most effective treatments include the use of in-shoe heel and arch cushioning with calf-stretching exercises and night splints that stretch the calf and plantar fascia while the patient sleeps. Prefabricated or custom-made foot orthotics may also alleviate fascial tension and symptoms. Other treatments may include activity modifications, NSAIDs, weight loss in obese patients, cold and ice massage therapy, and occasional corticosteroid injections. However, because corticosteroid injections can predispose to plantar fasciosis, many clinicians limit these injections. For recalcitrant cases, physical therapy, oral corticosteroids, and cast immobilization should be used before surgical intervention is considered. A newer form of treatment for recalcitrant types of plantar fasciosis is extracorporeal pulse activation therapy (EPAT), in which low-frequency pulse waves are delivered locally using a handheld applicator. The pulsed pressure wave is a safe, noninvasive technique that stimulates metabolism and enhances blood circulation, which helps regenerate damaged tissue and accelerate healing. EPAT is being used at major medical centers.

Surgical Treatment
Surgery should be reserved for patients who have made every effort to fully participate in conservative treatments, but continue to have pain from plantar fasciitis. Patients should fit the following criteria. Symptoms for at least 9 months of treatment. Participation in daily treatments (exercises, stretches, etc.). If you fit these criteria, then surgery may be an option in the treatment of your plantar fasciitis. Unfortunately, surgery for treatment of plantar fasciitis is not as predictable as a surgeon might like. For example, surgeons can reliably predict that patients with severe knee arthritis will do well after knee replacement surgery about 95% of the time. Those are very good results. Unfortunately, the same is not true of patients with plantar fasciitis.
Stretching Exercises
Stretching your plantar fasciitis is something you can do at home to relieve pain and speed healing. Ice massage performed three to four times per day in 15 to 20 minute intervals is also something you can do to reduce inflammation and pain. Placing arch supports in your shoes absorbs shock and takes pressure off the plantar fascia.